This is an interactive article, which is supposed to be read in a browser.
The crops begin even before the Fresno city limits end: rows of neatly pruned trees and bushes and vines incubating almonds, pistachios, cotton, tomatoes, plums, peaches, nectarines, oranges, lemons, grapefruits, mandarins and grapes—for eating, for drinking, for drying into raisins. This bounty is trucked hundreds or thousands of miles across California and the country, away from Fresno. The irony of life in the San Joaquin Valley is that locals rarely benefit from their region’s abundance. Almost 1 in 5 residents don’t reliably have enough to eat.
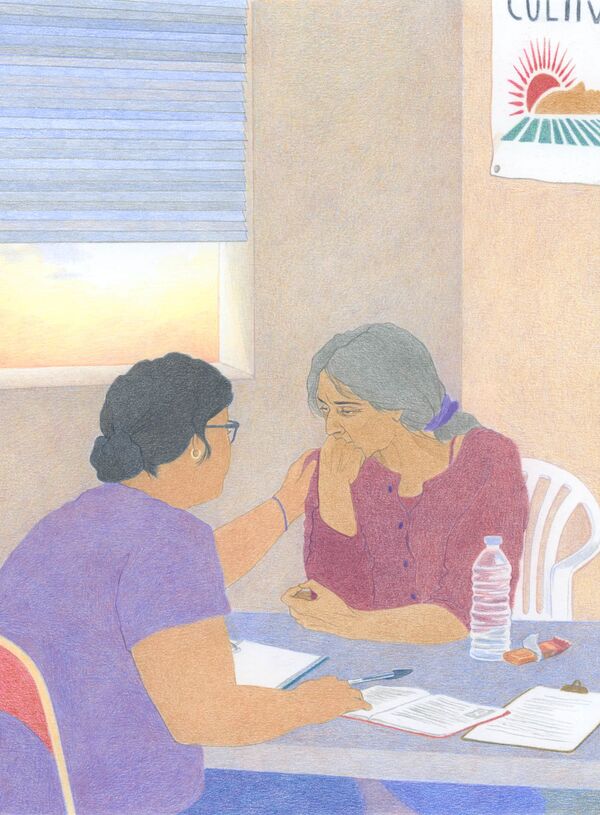
Among them is 76-year-old Señora Flores, who on this March morning is dressed in an elaborately appliquéd turquoise cardigan and matching tank top, her long gray hair secured with a satin scrunchie at the top of her head. She limps into the waiting room for a 9 a.m. appointment, already weeping from some combination of exhaustion, hunger, thirst, pain and heartache. It’s not quite clear when she last ate, but it wasn’t today. She drops heavily onto a small couch in the waiting room and tries to catch her breath.
The woman she’s meeting, a community health worker at a small nonprofit called Cultiva la Salud , had offered to come to her home, knowing that Flores doesn’t have a car and Fresno’s bus system is spotty at best. (Staffers refer to their clients using courtesy titles; Flores’ name has been changed to protect her medical privacy.) Yet Flores preferred to walk 1.6 miles south on Fresno Avenue, lugging a large cheetah-print tote bag stuffed with documents that have bedeviled her for weeks. The trip took her an hour and 45 minutes. When the receptionist hands her a pint-size bottle of water, she holds it to the sky, whispers “ Gracias, Padre ,” and sips.
A woman in false eyelashes and Doc Martens arrives to escort Flores to a cinderblock meeting room, then runs to grab a second water, an apple and a two-pack of granola bars out of a staff kitchen as Flores pulls her papers out of the tote. The pair settle in for what will become a two-hour session covering almost every aspect of a troubled life.
The very fact that this meeting is necessary incriminates the US healthcare system, whose labyrinth of unaffordable bills and unavailable appointments can seem designed to prevent people from getting the treatment they need. Livia Alejo, 37, the woman now whispering “ Dios mío ” as Flores explains her situation through tears, isn’t a doctor, a nurse, a therapist, a government employee or an insurance representative. As a community health worker, she’s simply trying to make up for the systemic failures of all five.
Alejo, who moved from Mexicali, Mexico, to Fresno in middle school, sometimes struggles to describe what she does in this office and in living rooms around the city and the surrounding farmland. Even the official definition of “ community health worker ” from the American Public Health Association equivocates to the point of meaninglessness: “a trusted member of and/or has an unusually close understanding of the community served” who serves “as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery.”
The job is just so many things at once—translator, advocate, case manager, paperwork wrangler, digital guide, health coach, detective. Alejo works with 17 patients at a time; as the supervisor of Cultiva’s team, she’s indirectly in charge of more than 100. After five years, she’s fluent in every element of the social safety net for Fresno residents. She knows who to call when the state’s public insurance system hasn’t sent someone their ID card, where to find doctors accepting new patients, which nonprofits still have money for rental assistance this month, where to get food after benefits run out and which programs will rule out undocumented immigrants. Solving one problem often means uncovering several more basic ones, as if she’s trying to sew a dress but first has to spin raw fiber into thread. “We’re the source of the resources,” Alejo says. “We have to find what is missing.”

The payoff from programs such as Cultiva la Salud can be something close to magic. Peer-reviewed research has found that community health workers can lower blood sugar in diabetic patients, lower blood pressure in hypertensive ones and lower cholesterol in hyperlipidemic ones. Patients who get support from community health workers smoke fewer cigarettes, get more exercise and rate their mental health more positively.
Better yet, these advocates know how to deliver care in a cost-effective way—not just for clients but also for health insurers and governments. By keeping people fed, housed and out of the hospital, community health workers, earning an average salary of $51,000 a year, are arguably the most cost-effective part of America’s healthcare system. One study found that every dollar invested in community health worker programs results in a $2.47 return for Medicaid. As a result, they’ve long been popular with Republicans as well as Democrats. GOP senators including Thom Tillis, Lisa Murkowski and Bill Cassidy have sponsored bills designed to increase the number of community health workers serving rural areas.
But though Cultiva and its peers save both lives and money, though they are both effective and well-liked, they are now also under unprecedented threat. They were among the hardest hit programs when the Trump administration canceled $12 billion in federal public health grants in the spring of 2025, and subsequent budget cuts at the National Institutes of Health and the Centers for Disease Control and Prevention delivered more blows. Cultiva was forced to lay off half its staff of 12 community health workers, and the total number serving the Fresno area dropped from 60 to about 25, says Joe Prado, the county’s public health director.
As of 2023, 58,500 Americans were employed as community health workers (sometimes called promotoras ), according to data from the US Bureau of Labor Statistics. Because of the fragmented nature of the workforce, it’s not yet clear how many of those jobs were lost once the funding cuts began in 2025. But one paper found that state and local public health organizations would lose about 45% of their grant money in 2026.
Alejo practically sparkles when she talks about helping clients like Flores. She’s always felt pulled toward supporting older people. Turning that passion into a career, even a stressful and underpaid one, felt like a dream. But she says she worries about how long she’ll get to do it. The grant that’s funding Cultiva’s remaining community health workers expires at the end of this year.

Getting Flores to this meeting required a series of intentional steps. A neighbor had handed her a flyer, picked up from a community fair, advertising Cultiva’s free monthly grocery box for low-income seniors in Fresno. Flores called to sign up, so Alejo dropped off the food. Standing on her doorstep, Flores mentioned she was afraid she was about to be kicked off Medi-Cal, California’s healthcare system for low-income residents. That was the moment Alejo had hoped for; it was the reason she’d made the delivery herself. She suggested they meet to figure it out together.
As soon as they sit down, Alejo can tell that potential ejection from Medi-Cal isn’t Flores’ most urgent issue. She needs mental health treatment, and soon. She can stop crying only for a couple of minutes at a time. Her daughter, who lives thousands of miles away, is seriously ill with kidney disease. Her husband died last year, leaving her bereft and with a new level of financial instability. Flores, who grew up in El Salvador, is a legal US resident with temporary protected status—which shields her from deportation because of instability in her home country—but that designation expires in September, and the Trump administration is working to end TPS for citizens of several other countries. “My heart and my soul are tired, very tired,” she says in Spanish, before unspooling an extended, enigmatic analogy about how God causes roses to bloom.
Alejo listens carefully, occasionally offering a tissue or murmuring consolations. She doesn’t interrupt or try to fast-forward to practical steps, even when Flores’ train of thought becomes difficult to follow. For now she’s focused on earning trust.
As a person with an official, unfamiliar title, Alejo also knows she is starting at a disadvantage. Tens of thousands of people in the Fresno region don’t have legal status; brutal US Immigration and Customs Enforcement sweeps in other cities during the second Trump administration have shrouded California’s Central Valley in fear. People here don’t open the door to strangers, literally or emotionally.
Like many immigrant children, Alejo served as her parents’ translator for years. When she was in college at Fresno State, she escorted her father to the hospital after an accident on the job. He’d asked a doctor about his periodic fainting spells, but the clinic never even tested his blood sugar, Alejo says. By the time they diagnosed him with diabetes, the disease had advanced so far that he died within a month. The hospital never offered a Spanish-speaking doctor or translator, or anyone to tell Alejo’s mom in her native language that her husband had died. Alejo had to do it. “My family needed someone to advocate for them and to be able to explain their needs to other people,” she says. “And I didn’t know where to look. I didn’t have a person who could guide me and help me find resources to help my dad.” After that, becoming that guide was all she ever wanted to do.
Alejo has blocked off two and a half hours for this appointment, standard for a Cultiva intake meeting. She and the community health workers who report to her know most of their clients are used to being ushered through an overburdened public clinic in 10 minutes, maybe getting handed a scribbled prescription on their way out. They evaluate every new client along 21 “pathways,” including food security, health insurance, transportation needs, medical screenings, education and employment. Any pathway they identify as an area of concern is added to the case file, with specific follow-up steps. Just getting through the screening questions can take more than an hour even with a client who provides straightforward answers, which Flores doesn’t.
As Flores pulls documents from her bag—reenrollment letters, bills, explanations of benefits, appointment reminders, prescriptions—Alejo notices that almost all of them are exclusively in English, like the ones her dad received about two decades ago. They’re also studded with terms too technical for most people to grasp in any language. Even after five years in the job, Alejo occasionally blinks in confusion at a line and turns to her laptop to google what these government and corporate bureaucracies are trying to say.
Within a half-hour, she pieces together what’s happened. A phone representative had told Flores she couldn’t book any medical appointments for April or May, because her Medi-Cal was set to expire at the end of March. That was a technicality; she met all the qualifications to reenroll and just needed to fill out the correct form. But the person on the phone hadn’t told Flores that, or hadn’t told her in a way she understood, and she hadn’t understood the letter that arrived at her home saying she needed to apply again. She panicked, sure she was about to stop getting her medication, sure the clinic wouldn’t let her in the door for the appointments she scheduled months ago. Her shoulders shake as she explains all this. Her sniffles turn into sobs. Step 1, Alejo sees now, is to fill out the reenrollment paperwork. She’ll return to the mental health question later.
For reasons relating to language, literacy, red tape and corporate dysfunction, millions of poor Americans either aren’t insured despite being eligible or don’t see a doctor regularly. When people don’t receive preventive care, they’re more likely to rely on the emergency room, which in turn costs local, state and federal governments more: Hospitals are required to treat patients regardless of their ability to pay, and hospital care is more expensive to provide. Prevention is cheaper than a cure. And Fresno’s economy is dependent on immigrants—many of whom have a temporary visa like Flores, or no legal status—so kicking them all out or refusing to treat them would cost money too.
A sea of peer-reviewed research supports what Alejo is doing as she sits with Flores. Trust blooms from understanding, from not needing to explain the basic facts of one’s life. Studies have shown that shared lived experience allows community health workers to boost screening rates for breast cancer, cervical cancer and colorectal cancer, and to increase access to primary care and follow-up appointments after hypertension diagnoses. As a result, patients with multiple chronic conditions spent 69% less time in the hospital when they received support from a community health worker, according to research published in 2018.
Once such workers have gained patients’ trust, they must then figure out what to do with it, says Shreya Kangovi, a physician in Philadelphia who’s written many of the most-cited papers on community health worker effectiveness . She now runs a company that builds infrastructure and training for community health worker programs. The worst programs, her research has found, focus on what she calls screen-and-refer work: “You know, ‘Mrs. Jones, do you have enough food to eat? Here’s the number to the food pantry.’ People know where the food pantry is!” Deeper problems are keeping them hungry.
In India, where Kangovi grew up, “we would never dream of having clinicians play both offense and defense.” Community health workers, who’ve been a core part of the country’s healthcare system for hundreds of years, take a proactive approach, helping people address the “social determinants” of health: food, housing and social support, all of which can make people either healthier or sicker. Doctors get involved when treatment is required, which happens less frequently when there’s a team playing offense.
The US has always underperformed on the offense side of healthcare. Even before the Trump budget cuts, few experts thought community health programs were being funded to their full potential. A sustainable, cost-effective system wouldn’t rely on the whims of the executive branch at all; community health workers would be thought of like doctors and nurses, so integral a part of the healthcare economy that they’d never again need to apply for one-year grants.
“There’s always a timeline for grants, a beginning date and an end date,” says Timothy Callaghan , a health policy scholar at Boston University who’s studied community health worker programs. “You might do everything right as a community health worker, but you lose your role anyway because the grant ends and there’s no new grant.” Cultiva la Salud is applying to become an authorized Medi-Cal provider, which would allow it to bill its community health workers’ salaries directly to the state, but no one knows how long that process will take.
Alejo understands she can’t solve everything for Flores. At the root of her clients’ diverse problems is a unifying one: They’re poor in a country where life often punishes people for being poor. Flores didn’t work enough years to qualify for Social Security; she retired in 2010 after complications from a long illness that almost cost her a kidney. She’s still grieving her husband and suffering from the knowledge that her daughter is sick thousands of miles away.
What Alejo can do is blunt the effect of all these indignities and do the heavy lifting to make someone’s life a little easier. Before last year’s layoffs, her team was doing it for twice as many people.
After this meeting, Alejo will leave the work at work, try to be satisfied with doing her best for the day and move on. She’s practiced this skill ever since her social-work internships in college. Blasting music on her way to the job helps. But here, poring over documents in this small cinderblock office, there’s only Flores. Alejo’s phone vibrates and flashes constantly while on silent. She never even glances at it.

The simple task of filling out Flores’ reenrollment paperwork introduces another challenge: She doesn’t have an email address and doesn’t know how to set one up, and without email, enrolling in any government benefit can take weeks. Alejo signs her up for Gmail, narrating the process aloud in Spanish to keep her client involved, then creates an account on benefitscal.com, California’s portal for safety-net services. Within a few minutes, the two have filled out the necessary form to renew Flores’ health insurance. Now they can investigate the status of her upcoming appointments.
Flores has already booked an annual primary care exam and a mammogram, meaning she’s more on top of things than many Americans, but she doesn’t know if the appointments are still valid. Alejo suggests they call together to find out. Although Medi-Cal is Flores’ insurance provider, in this case she needs to call CalViva Health, its Central Valley subsidiary.
That Flores has insurance at all gives her advantages over many of her neighbors. At the same time that budget cuts have annihilated community health worker programs, changes to other programs have made it more difficult for many poor people in Fresno to get insured. The Trump administration’s One Big Beautiful Bill Act rolled back rules that streamlined Medicaid enrollment and renewal processes, and implemented work requirements that will start in 2027. California, meanwhile, “paused” noncitizens’ eligibility for full-coverage Medi-Cal starting on the first of this year. Flores is grandfathered in, but 3 million fewer Californians are expected to be enrolled in Medi-Cal by 2028. “Right now the dominant narratives are about how there are people in our country who don’t belong here,” says Genoveva Islas, Cultiva’s founder and executive director. “We’re in a very different situation than I’ve ever seen before in terms of the antagonism, even when it actually costs money.”
CalViva, which serves a region where more than half the population is Latino, makes it easy to talk to someone in Spanish: “ Para continuar en español, oprima el dos ” is the second sentence the recorded voice offers. Within 30 seconds, Alejo is connected to a woman who introduces herself as Elizabeth.
Alejo speaks first, saying she’s with a client who has questions about her coverage. This throws Elizabeth off: “Ummmm, excuse me, who are you?” A community health worker helping Flores, Alejo says. “OK, can I speak with her? Please take me off speakerphone.” Alejo follows the directions, instructing Flores to speak into the phone’s mouthpiece. This plan lasts a matter of seconds. Elizabeth needs Flores’ membership number, and Flores doesn’t know where to find it. Alejo switches back to speakerphone and stays silent, copying the numbers Elizabeth is asking for from Flores’ enrollment paperwork in big block letters so Flores can read them aloud.
It’s an inefficient system, but it works. Elizabeth soon confirms that Flores still has a mammogram scheduled during the last week of April and a primary care appointment in mid-May, both of which Medi-Cal will cover.
Any distrust Flores felt for Alejo earlier this morning is long gone; her list of illnesses and fears pours out of her like water from a toppled glass. Alejo tells her client she’s very grateful she’s sharing her worries, but Flores cuts her off. “I’m not even telling you everything, because people say, ‘This old woman is crazy.’ I’m not crazy!”
Sometimes Flores has to stop talking long enough to catch her breath, but then she’s right back to it. She explains her daily medication schedule: one pill at 8:30 a.m. and again at 8:30 p.m., a different one at 10:30 a.m., two more at noon and one at 2 p.m. She’s religious about taking them on time, in part because she’s religious in the traditional sense: “There are so many things only God knows, but God is here. That guides me and gives me the strength to accept my illnesses,” she says, then turns her eyes to the heavens. “You have the power and the strength to cure me.”
“Amen,” Alejo adds. “Or to keep you healthy for the moment.”
The reality is that a “cure” is not the goal for a 76-year-old with multiple overlapping chronic conditions. Flores is most concerned about her diabetes; her blood sugar has been skyrocketing recently, which keeps her in bed much of the time. Sometimes her heart races so fast she feels as if it’s going to escape her chest. She worries her medicines aren’t working anymore.
Type 2 diabetes is the single-most-common condition among Alejo’s patients. Latinos are 80% more likely than White Americans to have diabetes, which researchers attribute to a mix of genetic factors such as higher insulin resistance and sociocultural ones like lower average income. These demographic factors have made diabetes an area of particular interest for community health worker programs and the researchers who study their effectiveness. Multiple peer-reviewed studies have shown that community health workers can successfully treat diabetes by coaching patients to monitor their blood sugar, take their medications, get more physical activity and eat more healthily. A 2025 literature review found that patients under the care of a community health worker for at least 12 months saw a clinically significant 0.5-point reduction in their blood sugar.
Alejo has no interest in broaching the subject of lifestyle changes at this meeting. Flores seems to be hanging on by a thread; prescribing more exercise feels beside the point. Community health work is so often a matter of triage, and Alejo is an expert at judging in the moment what actually demands her attention.
What this moment requires, she sees, is ensuring Flores is under regular medical care. Flores recently switched to a new primary care doctor, whom she likes much better than the last—she didn’t feel he took her concerns very seriously. Hearing about the new doctor makes Alejo beam. She can still picture the moment almost 20 years ago when a nurse whispered to her that she had the right to ask for a different provider for her dad, who was being disrespected. Alejo asks every client whether their doctor treats them well. If the answer is no, she’ll call to coordinate a switch herself.
The optometrist is another story. Diabetes is starting to claim Flores’ eyesight. When Alejo asks for her signature on a form allowing a Cultiva employee to make calls on her behalf, Flores struggles to find the line for her name. She had cataract surgery recently, which insurance covered, and she pulls a prescription for glasses from the stack of papers she’s got in her cheetah-print bag. The doctor told her that Medi-Cal wouldn’t cover the glasses, and the cheapest ones she saw for sale at his office were $1,200, which she doesn’t have. She’s planning to go to Walmart tomorrow to check the prices; she thinks glasses cost more like $700 there, which is still too much, but the store offers payment plans.
Alejo looks stricken by the idea of Flores taking out a high-interest loan just to afford the glasses she needs. “You qualify for free glasses through Medi-Cal,” she says firmly. “I will make a call.”
She jots down a note to follow up on the glasses, then turns to figuring out how to get Flores regular access to food. This, too, will benefit taxpayers as well as her client. Food insecurity and additional spending on healthcare are deeply intertwined problems: One paper showed that in California alone, not having enough to eat resulted in $7.2 billion in additional healthcare costs in 2016. Delivering groceries to low-income people is a logical first step, but food alone can go only so far , according to a small pilot study published earlier this year. What really made a difference in outcomes, and thus in costs to the government, was giving people both food and access to a community health worker. The combination resulted in a reduction in blood sugar from 8.4% to 6.7% among diabetic patients after six months, which can mean the difference between needing insulin or not.
California residents with temporary protected status don’t qualify for CalFresh, the state food assistance program. The boxes Cultiva packs for low-income seniors are delivered only once a month. Alejo knows every soup kitchen in the area, and which ones are closest to Flores’ home, but “close” is a relative term in sprawling Fresno. Even if this frail woman was able to walk to a site once a week, how would she carry the groceries home? There’s a delivery service called Project FoodBox, but they just serve people with private insurance, not Medi-Cal.
Alejo has an idea for how to fix this problem too. She’ll scour Facebook Marketplace to see if anyone is giving away some sort of dolly or cart that she can bring to Flores. If that doesn’t work, she’ll come up with something else. But all of that will have to wait until later, after she’s typed up her notes, called Medi-Cal about the glasses, checked on her staff and seen her other clients.
Before she gets to any of that, though, Alejo needs to talk to Flores about getting into therapy.
She has plenty of experience with this delicate conversation. Depression and anxiety are common among her older clients, all of whom carry the weight of some combination of poverty, hunger, loneliness, immigration fears, physical disability and chronic health conditions. But that’s not to say it always goes well. Latino immigrants are less likely than White Americans to attend therapy or see a psychiatrist, even when their insurance covers it, which Flores’ CalViva plan does. Sometimes people insist they’re doing just fine, even when Alejo can tell they’re not. Sometimes they tell her they’ll call to schedule an appointment when they get home, even when she knows they won’t.
Alejo cares about this woman. She wants her to see a counselor for the same reason she wants her to get her mammogram: She believes people shouldn’t die from treatable diseases even if they’re poor, even if they’re not citizens. But even measured in the most mercenary terms, using Medi-Cal funds to get Flores mental health care is a good investment. People with mental health issues get sicker from heart disease and other chronic conditions, which means they stop working or need costlier treatment. McKinsey & Co. researchers have found that each dollar spent on mental health interventions yields an economic return of at least $5.
After an hour in this room, Alejo is ready to push the issue. Flores is crying again. Her heart hurts, she says several times. “I’m so sorry that you’ve gone through this,” Alejo says. “And of course you can talk to a counselor, to a therapist. You have the right. We can make an appointment, if you like.”
Flores seems surprised by this news. She did ask about seeing a therapist once, she says, but her former doctor told her she didn’t require treatment. “I need it more than you do,” she remembers him saying. Alejo suggests they call to get a referral.
Even if she had known she qualified for free therapy, Flores wouldn’t have been able to handle this call alone. A CalViva “customer service advocate” named Veronica answers the phone right away, but she just speaks English, with a thick Southern drawl. Alejo asks to be connected to a Spanish speaker, but there are no customer service advocates who speak Spanish. There are interpreters, but Veronica needs to talk to Flores first. “Good afternoon, my name is Veronica, and I’m a customer service advocate. Are you needing a Spanish interpreter?” she asks. Alejo translates, and Veronica accepts Flores’ “ Sí ” as confirmation.
The interpreter, who introduces himself as Alejandro, manages to grease the skids only slightly. He repeats Flores’ full name, but Veronica struggles with the spelling, asking him to repeat each letter multiple times. This goes on for two excruciating minutes. Veronica has difficulty finding Flores’ account using either her name or member number. Then she needs an email address, which Flores doesn’t know because it’s existed for less than an hour. Alejo, attempting to stay silent because Veronica seems thrown by her presence, writes it down, pointing to each letter as Flores reads them aloud.
Finally, Veronica is ready to begin the questionnaire that will allow her to refer Flores to a therapist. When she asks about the reason for the call, Flores answers without hesitation: “Sometimes I feel confused, and I get panicked from sadness and crying. I don’t know the reason,” she says. “Sometimes I prefer to isolate myself, because I don’t feel comfortable around other people. I can’t come to church anymore, because I can barely walk and I’m in pretty bad health.”
Asked if she’s suicidal, Flores is emphatic. “No, I don’t want to take my own life,” she says. “But sometimes I feel afraid of falling asleep and not waking up.”
Forty minutes after the call began, Alejo and Flores get what they came for: the names of three local mental health providers who accept CalViva insurance, speak Spanish and are, at least theoretically, accepting new patients. That’s not to say they’re convenient for Flores, though. The closest one is a few blocks from the Cultiva office, about 1.5 miles from Flores’ home. Alejo immediately starts wondering how Flores will make the journey and whether there’s some way she can take her.
After they hang up with Veronica and Alejandro, Flores’ voice is noticeably lighter. Alejo asks whether she wants help calling the therapists or an escort to her doctors’ appointments, but Flores says confidently that she can handle it. Looking intently at Alejo, she offers a brief prayer: “I place into your hands all the people you bring into my life. May no harm befall them; may you continue to watch over and protect them. And I ask God—I ask my Father from the bottom of my heart, in the name of Christ Jesus and through the glory of his Holy Spirit—to grant them all the desires of their hearts.”
On the other side of the office, Islas, Alejo’s boss, is fretting about how to keep Alejo’s team employed. Across the country, nonprofits and philanthropic leaders are trying to find ways to fill the gaps created by federal funding cuts. Some local governments have set up emergency funds to keep community health programs up and running, and community foundations have created new lines of funding. But all of these measures put together still aren’t enough to replace the financial might of the federal government. Even the most generous grants expire. “In an environment where resources are shrinking, decisions have to be made in healthcare systems about where to cut, and chances are they’re not going to want to cut doctors or nurses or social workers,” says Callaghan, the health policy scholar. Community health workers are the ones to go. “As you lose those community health workers, you’re losing those connections they provide, and the result is less access to care.”
Alejo is trying not to think about any of this. She has about an hour to write up her notes from the meeting and check in with her team about how things are going with their clients. One is on her way to an intake appointment at the home of another older woman who doesn’t have enough food. After she eats lunch, Alejo will set off to meet an undocumented couple she’s known for months; they need help applying for emergency rent assistance so they don’t get evicted.
She knows she’s made a measurable difference in Flores’ life over these two-plus hours. She’s built a relationship that will allow her to work with the woman for years: bringing her food, untying the Medi-Cal knots, connecting her with other services, watching the progress she makes in therapy, helping her live a longer and better life.
She’ll get to do all that, that is, if the money doesn’t run out.
The two women embrace for several seconds before Flores sets out for the long walk home. Alejo promises to call soon to check in.